

Patient Intake Procedures: Essential Definitions & Processes
Patient intake is where healthcare operations either gain control or lose it. A weak intake process creates downstream errors in scheduling, eligibility, documentation, coding support, patient flow, and compliance — and those failures compound by the time the chart reaches the clinician. A strong intake process, by contrast, turns the front end into a clinical and administrative quality filter.
This guide breaks patient intake into practical definitions, role-based steps, failure points, and process standards that medical administrative teams and scribes can apply immediately. If your team is battling repeated demographics errors, insurance rework, delayed rooming, missed authorizations, or inconsistent handoff notes, this is exactly where to fix it.

1) What Patient Intake Actually Means in Modern Healthcare
“Patient intake” is not just “checking a patient in.” It is the structured process of collecting, verifying, normalizing, documenting, and routing patient information before clinical care, during arrival, and at transitions in the visit. In real operations, intake spans phone calls, portal submissions, pre-registration, front desk workflows, triage handoffs, EMR data entry, consent capture, and financial communication.
For ACMSO learners building healthcare readiness, intake proficiency overlaps directly with medical office workflow fundamentals, EMR terminology fluency, scheduling systems knowledge, patient management platforms, and data privacy expectations for healthcare admin roles.
Core definition
Patient intake is the front-end data capture and validation process that prepares a patient encounter to be clinically safe, operationally efficient, financially billable, and legally compliant.
That definition matters because many teams only focus on speed. Speed without validation produces rework. Rework destroys throughput. Throughput failures increase wait times, frustrate patients, and make staff appear disorganized even when they are working hard. This is why teams pursuing stronger administrative performance often pair intake optimization with medical administration efficiency insights, medical office automation trends, future EMR system changes, and healthcare administration trend reports.
Why intake is a high-stakes process, not a clerical formality
A single intake error can trigger multiple downstream consequences:
Wrong DOB or subscriber ID → eligibility denial risk
Wrong pharmacy listed → refill delays or callbacks
Missing allergy entry → safety risk and incomplete chart support
Incomplete chief complaint wording → weak triage prioritization
Missing consent documentation → compliance exposure
Uncaptured contact preference → failed reminders and no-shows
Duplicate chart creation → fragmented documentation history
These are not isolated “front desk mistakes.” They are system design failures. Teams that understand this treat intake the same way high-performing organizations treat documentation accuracy standards, healthcare documentation trend shifts, compliance-sensitive workflows, and medical scribes’ role in new standards navigation.
Key intake domains every admin team must manage
Patient intake can be organized into six operational domains:
Identity & demographics (legal name, DOB, sex, address, contact details)
Coverage & financial clearance (insurance, eligibility, authorizations, guarantor)
Clinical context capture (chief complaint/reason for visit, history prompts, meds/allergies depending on workflow)
Consent & compliance (HIPAA/privacy acknowledgment, treatment/financial forms, notices)
Operational routing (provider, location, appointment type, rooming/triage pathway)
Communication preferences (language, interpreter need, SMS/email reminders, portal)
Mastering these domains improves performance in both CMAA and scribe pathways, especially for learners working through CMAA career roadmaps, top CMAA skills employers want, medical scribe employer-ready skills, and career pathways from entry-level to leadership.
| Intake Term / Step | What It Means in Practice | Why It Matters (Operational Impact) |
|---|---|---|
| Pre-registration | Collecting demographics/insurance before visit date | Reduces front-desk congestion and late starts |
| Patient registration | Creating or confirming the patient record | Prevents duplicate charts and identity errors |
| New patient intake | Full data capture for first-time encounters | Builds baseline record for all future visits |
| Returning patient check-in | Updating existing record and visit details | Keeps records current and billable |
| Demographic verification | Confirming legal name, DOB, address, contact data | Avoids misidentification and claim issues |
| Insurance capture | Entering payer, member ID, group, subscriber details | Supports eligibility and clean claims |
| Eligibility verification | Checking active coverage and benefit status | Prevents avoidable denials and surprise balances |
| Authorization check | Confirming prior auth/referral requirement | Reduces delayed care and nonpayment risk |
| Referral validation | Ensuring referral source/order matches visit type | Prevents scheduling and reimbursement mismatch |
| Chief complaint | Patient’s primary reason for the visit | Drives triage priority and documentation flow |
| Reason for visit (RFV) | Operational phrasing for appointment purpose | Aligns scheduling slot with provider expectations |
| Medication reconciliation prompt | Prompting patient/provider to review med list | Supports safer charting and fewer discrepancies |
| Allergy verification | Confirming allergies/intolerances and reactions | Improves patient safety and alert accuracy |
| Preferred pharmacy | Recording patient’s pharmacy location | Prevents prescription routing delays |
| Consent to treat | Patient authorizes care delivery | Core legal/compliance requirement |
| HIPAA acknowledgment | Patient acknowledges privacy notice receipt | Supports privacy compliance documentation |
| Financial responsibility form | Patient acknowledges payment obligations | Reduces billing disputes and collection friction |
| Guarantor information | Responsible party billing details | Essential for minors/dependents and statements |
| Photo ID verification | Confirming identity with government/accepted ID | Reduces fraud and wrong-chart registration |
| Interpreter need screening | Identifying language assistance requirement | Improves access, safety, and informed communication |
| Contact preference | SMS/call/email and consent for reminders | Improves attendance and follow-up success |
| Portal enrollment status | Patient activated or pending portal access | Supports pre-visit forms and post-visit messaging |
| Arrival status | Marked arrived/checked-in in practice system | Triggers rooming and queue visibility |
| No-show / late policy acknowledgment | Patient informed of attendance policies | Reduces disputes and protects schedule integrity |
| Copay collection | Collecting patient-responsibility amount at check-in | Improves cash flow and lowers A/R burden |
| Clinical handoff note | Concise intake-to-clinical team transition details | Prevents missed context and queue confusion |
| Duplicate chart check | Searching for existing records before creation | Protects chart continuity and documentation accuracy |
| Intake timestamping | Recording when each intake action occurred | Supports audits, throughput analysis, accountability |
| Exception queue | Holding incomplete/problematic intakes for follow-up | Prevents silent failures and lost revenue |
2) Essential Patient Intake Definitions Every ACMSO Learner Should Master
If staff can’t define intake terms consistently, they cannot execute them consistently. One of the biggest causes of front-office chaos is vocabulary mismatch: one person says “registered,” another means “arrived,” another means “eligible,” and the provider assumes the chart is cleared. Precision language prevents operational ambiguity.
Professionals preparing for healthcare admin and scribe roles should build fluency through resources like medical administrative terminology mastery, top CMAA terms to master, the 100 most important medical administrative terms, the 100 most important terms for medical scribes, and EMR software term walkthroughs.
Definitions that directly affect intake performance
1) Registration vs. Check-in
Registration = creating/updating a patient record in the system
Check-in = marking the patient as arrived for today’s encounter
Why teams fail here: staff may complete check-in without finishing registration updates. Result: patient is “in queue,” but demographics/insurance remain stale. This leads to post-visit rework, claim edits, and callback cycles. Teams working toward stronger office execution often combine patient flow management training, scheduling software workflow literacy, medical office telephone etiquette standards, and active listening scenarios in healthcare.
2) Demographics validation vs. demographics entry
Entry means typing in what is provided
Validation means confirming it is current, complete, and standardized
Typing fast is not the same as validating well. If “St.” vs “Street,” wrong apartment unit, outdated phone number, or swapped subscriber fields remain uncorrected, downstream communication and claim accuracy suffer. This is why healthcare teams are increasingly pairing admin training with medical administration technology trends, automation opportunities for CMAAs, future healthcare compliance readiness, and HIPAA update preparedness.
3) Eligibility verification vs. benefits explanation
Eligibility verification confirms active coverage and payer data
Benefits explanation is communicating cost-sharing expectations (copay, deductible, etc.)
A common pain point: patients say “my insurance is active,” but the office never verified plan status for that specific date or service category. Another pain point: staff verify eligibility but never communicate financial expectations clearly, causing frustration at checkout. These are avoidable with structured workflows and healthcare administration efficiency practices, CMAA career growth skills, medical office automation frameworks, and predictive telemedicine admin insights.
4) Chief complaint vs. appointment label
The appointment label may say “follow-up,” “new patient,” or “consult.”
The chief complaint/reason for visit explains what the patient needs today.
If these diverge and no one catches it, scheduling length, rooming priority, documentation expectations, and provider prep all break. Scribes and admins who understand this alignment perform better in ER scribing environments, specialty documentation tracks like cardiology, orthopedic scribing workflows, and surgical documentation settings.
5) Intake completion vs. intake readiness
A form can be “completed” and still not be ready. Readiness means all required elements are accurate enough for the next team to act without rework.
This distinction is where mature teams outperform struggling ones. They build readiness checks into intake rather than pushing errors downstream to nursing, billing, or clinicians. If your clinic always feels “busy but behind,” intake readiness is often the hidden bottleneck — the same kind of systems issue highlighted in medical scribe clinical efficiency research, real-time healthcare administration insights, documentation accuracy reporting, and industry reports on data accuracy impact.
3) The End-to-End Patient Intake Process (From Appointment Creation to Clinical Handoff)
A high-performing intake process is not one step — it is a sequence of controlled checkpoints. Most failures happen at transitions: call center to scheduler, scheduler to pre-reg, pre-reg to front desk, front desk to triage, triage to provider, provider to checkout/billing. Your goal is to reduce ambiguity at every handoff.
Teams building operational maturity often benefit from seeing intake as part of a larger ecosystem that includes patient management systems, EMR platform knowledge, AI/automation shifts in healthcare documentation, and the future of medical documentation in AI-driven workflows.
Stage 1: Appointment intake (before the patient ever arrives)
This is where many clinics already lose accuracy.
What should happen
Confirm patient identity (new vs returning)
Capture/confirm contact details
Define appointment type and reason for visit
Collect insurance basics and referral/auth requirements
Flag special needs (interpreter, mobility support, paperwork load)
Send pre-visit forms/portal instructions
Common pain points
Appointment booked under wrong provider/template
“Follow-up” scheduled when issue is new/urgent
Referral required but not identified until check-in
Patient never receives forms due to wrong email/mobile
No pre-visit instructions for fasting, records, arrival time
These breakdowns raise no-show risk, increase lobby wait times, and force staff into reactive mode. Operationally, this is why teams increasingly rely on interactive job-demand and workflow reports, virtual medical administration process changes, telehealth regulation readiness, and telehealth role transformation insights.
Stage 2: Pre-registration and insurance readiness
This stage separates smooth clinics from chaotic clinics.
High-value process controls
Run eligibility verification before date of service
Validate subscriber/guarantor details
Confirm referral and prior auth status
Identify coverage mismatches early
Create exception queue for unresolved cases
Contact patient before visit if action is required
When teams skip this stage, they create same-day intake crises that front desk staff cannot resolve quickly under pressure. Patients experience “you should have told me earlier” moments. Staff experience blame for problems caused upstream. This is exactly the kind of preventable friction that CMAA workforce trend reports, job security and salary growth data tied to certification, annual job market reports, and career progression interactive reports indirectly reward — because stronger process reliability gets noticed.
Stage 3: Arrival and check-in execution
At arrival, the team must balance speed, empathy, privacy, and accuracy.
Minimum check-in sequence
Greet and identify patient using approved identifiers
Confirm appointment/provider/location
Verify demographics and contact changes
Capture insurance card/ID updates
Confirm forms/consents
Collect copay (if policy/workflow requires)
Mark arrived/check-in status correctly
Route chart to next queue/team
Why this stage collapses in many offices
No standardized script
Too many clicks in EHR/practice system
Staff multitasking phones + walk-ins + portals
Patients completing forms in lobby at the last minute
Missing scanning/upload conventions
Unclear ownership for unresolved issues
To reduce this, combine administrative scripting with conflict resolution scenarios for medical admin, patient advocacy communication skills, telephone etiquette standards for spillover calls, and office ergonomics/safety workflow planning.
Stage 4: Clinical-context intake and pre-rooming handoff
Depending on the setting, front-desk or intake staff may capture:
chief complaint / reason for visit
medication/allergy updates
pharmacy confirmation
basic questionnaires (screening, forms, specialty-specific prompts)
In scribe-supported clinics, intake quality directly affects how quickly the documentation workflow stabilizes once the provider enters. That’s why intake excellence has a measurable link to medical scribe impact on hospital revenue, clinical documentation enhancement roles, patient care coordination improvements, and compliance/documentation standards navigation.
Stage 5: Exception handling and escalation
A professional intake team is not judged by how they process perfect cases — they are judged by how they handle exceptions without breaking flow.
Examples of intake exceptions
Patient in wrong location
Insurance inactive or plan changed
Missing referral/auth
Name mismatch between ID and insurance
Portal forms incomplete
Duplicate chart suspected
Urgent symptoms reported at check-in
Interpreter needed but not scheduled
Create a simple escalation matrix:
Front desk resolves (demographics/contact updates)
Financial clearance resolves (eligibility/auth/referral issues)
Clinical triage resolves (symptom urgency)
Supervisor resolves (identity conflict/duplicate chart/high-conflict scenarios)
That structure protects throughput and reduces emotional burnout — a theme echoed in interactive reports on burnout reduction through workflow support, healthcare facilities preferring certified scribes/admins, industry investment increases in scribes, and economic impact analyses of scribe-supported operations.
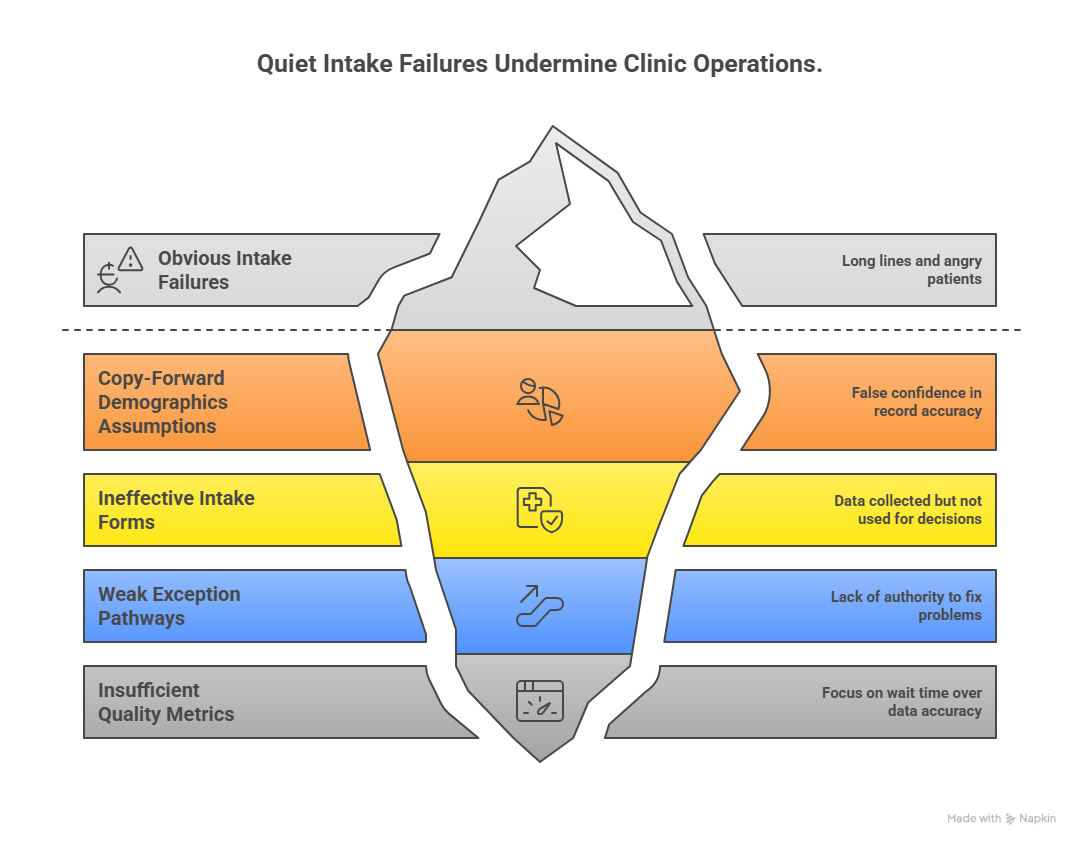
4) Patient Intake Failure Points That Quietly Damage Compliance, Throughput, and Revenue
Most clinics recognize obvious intake failures (long lines, angry patients, system downtime). The more dangerous failures are the quiet ones — errors that pass forward unnoticed and reappear later as denials, chart discrepancies, patient complaints, or provider dissatisfaction.
If your team feels like it is constantly “fixing things after the fact,” these are the failure points to audit first. ACMSO learners preparing for modern roles should also track how these risks connect to real-time compliance/documentation shifts, billing code changes that affect admin teams, data privacy readiness, and regulatory change timelines for CMAAs.
Failure point 1: “Copy-forward” demographics assumptions
Many offices assume returning patients need only a quick verbal confirmation. That works until:
the phone number changed
the address changed
insurance changed at the new year
guarantor changed for a dependent
preferred pharmacy changed
communication consent changed
The pain point is not just a stale field — it is the false confidence that the record is accurate. A better approach is structured re-verification prompts by data category, supported by patient management system workflows, EMR term fluency, medical billing software terminology understanding, and inventory/system process literacy where relevant to offices.
Failure point 2: Intake forms that collect data but don’t improve decisions
Some intake packets are long, repetitive, and poorly routed. Staff spend time collecting information that no one reviews before rooming. That creates a hidden trust problem: patients feel they completed “everything,” but staff ask the same questions again.
Fix:
Remove nonessential fields from day-of-visit intake
Separate legal/compliance forms from clinical screening forms
Route fields to the correct user/team
Build “required for today” vs “nice to have” logic
This is the same process-thinking that helps professionals succeed in medical office automation opportunities, technology preparedness for CMAAs, AI transformation of admin roles, and medical office of 2025 technology guides.
Failure point 3: Weak exception pathways
Intake teams often know something is wrong but lack authority or clarity to fix it. Example: front desk detects inactive insurance, but no same-day escalation path exists; patient waits, staff improvises, provider schedule slips, and billing team inherits a preventable problem.
Fix:
Define exception categories
Define owner by category
Define maximum wait-to-escalate threshold
Document disposition in system/notes
Train scripts for patient communication during delays
This kind of clarity is one reason certified professionals often advance faster in CMAA career opportunity pathways, real-life success story tracks, medical scribe certification career boosts, and medical scribe career growth trends.
Failure point 4: No intake quality metrics beyond “wait time”
Wait time matters, but it is not enough. A clinic can reduce check-in time while increasing bad data. Speed-only metrics reward shortcuts.
Add intake quality metrics such as:
demographic update completion rate
eligibility verified before arrival rate
missing consent rate
duplicate chart rate
check-in exception rate
same-day auth/referral failure rate
intake-to-rooming handoff defect rate
Teams that measure process quality become far more credible when arguing for staffing, training, or technology investments — similar to how data-backed positioning strengthens medical scribe workforce reports, employment trend visualizations, job market reports by specialty, and real-time employment predictions and reports.
5) Best-Practice Patient Intake Workflow Design (Scripts, Checklists, Roles, and Training)
A strong patient intake process is built, not hoped for. The highest-performing teams do four things well: standardize, prioritize, train, and audit. They don’t rely on “experienced staff just knowing what to do.” They create repeatable workflows that new staff can execute reliably and senior staff can refine.
This is exactly the professional edge ACMSO training paths aim to develop through exam prep and skills readiness, interactive CMAA practice testing, medical scribe certification prep guides, and medical scribe practice exam tools.
A) Build a role-based intake map
Do not put every intake responsibility on one person. Define role boundaries:
Scheduling team (pre-visit)
appointment type accuracy
preliminary insurance collection
visit instructions
portal/pre-form communication
Pre-registration / authorization team
eligibility verification
referral/auth tracking
exception outreach before visit
Front desk check-in
identity confirmation
demographics updates
ID/insurance scan confirmation
consent/financial forms
arrival status / queue routing
Clinical intake / rooming support
chief complaint refinement (within role scope)
med/allergy/pharmacy verification prompts
handoff note quality
Supervisor / lead
exception escalation
duplicate chart resolution pathway
KPI auditing and coaching
Role clarity reduces blame and improves training speed — a major advantage for teams hiring from medical scribe job growth markets, top cities hiring scribes, best cities for scribe careers, and medical admin job demand by specialty.
B) Use intake scripts that preserve empathy and precision
Scripts are not for sounding robotic. They are for ensuring nothing critical is missed under pressure.
Example identity + update script
“Before I check you in, I’m going to quickly confirm your name, date of birth, phone number, and insurance so your chart and billing stay accurate for today’s visit.”
Why this works:
signals purpose (accuracy)
reduces patient resistance (“why are you asking again?”)
sets expectation for a quick but structured verification
Pair communication scripts with active listening training, patient advocacy scenarios, conflict resolution frameworks, and telephone etiquette practice to improve patient experience while keeping pace.
C) Create a “minimum complete intake” checklist
A high-value checklist prevents rushed omissions.
Minimum complete intake checklist (day-of-visit)
patient identity confirmed using approved identifiers
demographics reviewed/updated
insurance/guarantor reviewed and scanned if changed
required consents acknowledged/captured
financial responsibility discussed per policy
reason for visit/chief complaint recorded correctly
arrival status updated
queue routed to correct next step
exception note documented if unresolved
This checklist works best when integrated into EMR workflow understanding, patient flow terminology frameworks, facility safety and emergency procedures knowledge, and medical office operational best practices.
D) Train for scenarios, not just forms
Many onboarding programs teach field names, but not what to do when reality doesn’t match the script. Scenario training should include:
patient disputes balance at check-in
insurance card missing / photo on phone only
urgent symptoms disclosed at front desk
language barrier and no interpreter pre-arranged
parent/guardian/guarantor mismatch
telehealth patient not portal-ready
duplicate chart suspected
incomplete referral on specialist visit
This kind of training makes staff visibly more competent and supports career growth in both admin and scribing tracks, including remote medical scribing transformations, telemedicine’s growing need for scribes, future evolution in scribe roles, and emerging specializations for medical scribes.
E) Audit intake weekly with a defect-based review
If you only coach staff when patients complain, you are training by crisis. Instead, audit a sample of encounters weekly.
Review for:
incorrect/missing demographics
incorrect insurance/subscriber data
missing required forms
wrong visit type
missing chief complaint specificity
duplicate chart near-misses
poor exception documentation
handoff delays caused by incomplete intake
Then link findings to targeted retraining using CMAA exam topic breakdowns, top exam mistakes to avoid, medical scribe exam breakdowns, and medical scribe exam mistake prevention.
6) FAQs: Patient Intake Procedures (High-Value, Real-World Answers)
-
Patient registration is the creation or update of the patient record; patient intake is broader and includes registration plus verification, consents, financial communication, visit-specific information capture, and routing to the next care step. If a clinic says “intake is complete” but only demographics were entered, the process is incomplete. This distinction becomes crucial in patient flow management workflows, EMR-driven office processes, medical admin efficiency systems, and future-proof administrative skill planning.
-
The biggest ones are stale demographics, unverified insurance, wrong appointment type, missing referral/auth checks, incomplete consent capture, duplicate chart creation, and vague reason-for-visit documentation. These errors usually surface later as denied claims, rooming delays, clinician frustration, or patient callbacks. Teams trying to reduce these failures should review documentation accuracy strategies, medical scribe compliance support insights, annual documentation trend reports, and data-accuracy impact reports.
-
Use pre-registration, role-based task separation, standardized scripts, and a minimum complete intake checklist. Speed improves when staff stop solving preventable same-day problems (inactive insurance, missing forms, wrong visit types). Focus on moving verification earlier and exceptions into a defined queue. This aligns with best practices discussed in medical office automation opportunities, technology guides for future-ready CMAAs, virtual medical administration workflows, and telehealth operations changes.
-
That depends on the practice’s workflow, scope definitions, and system design. In many settings, front desk staff may confirm/update limited information (e.g., preferred pharmacy, high-level reason for visit), while clinical staff handle deeper medication/allergy reconciliation. The key is clarity of role and handoff standards, not guessing. Practices with scribe support often see stronger continuity when intake aligns with medical scribe role best practices, essential scribe skills, AI-era documentation role evolution, and clinical documentation specialist pathways.
-
Track both speed and quality. Start with: average check-in time, pre-registration completion rate, eligibility-before-arrival rate, missing consent rate, duplicate chart rate, unresolved exception rate, intake-related rooming delay rate, and same-day referral/auth failure rate. Without quality metrics, teams optimize appearances instead of outcomes. Managers making staffing or training cases can strengthen decisions using medical administration workforce data, CMAA salary and advancement reports, job market demand reports, and career progression analytics.
-
Strong intake gives providers and scribes a cleaner starting point: accurate demographics, correct visit context, verified insurance/authorization status, and fewer interruptions caused by front-end corrections. That improves note flow, reduces repeat questioning, and protects patient trust. It also supports broader outcomes seen in clinical efficiency research, physician burnout reduction reports, economic impact analyses, and health systems investment trends in scribes.