

Remote Medical Scribing: Transforming Healthcare Documentation
Remote medical scribing is not a trend. It is a workflow upgrade that removes the biggest productivity tax in clinical care: unfinished documentation. When a remote scribe captures the visit in real time, providers stop carrying chart debt into the evening, coding teams stop chasing clarifications, and admin staff stop rebuilding the same information in three places. The result is faster sign off, cleaner claims, tighter compliance, and a calmer day for everyone. This guide breaks down what remote scribing really changes, how to implement it safely, and which metrics prove it is working.

1) Why Remote Scribing Is Reshaping Documentation Right Now
Remote scribing is winning because it attacks the hidden bottleneck that clinics keep tolerating: documentation drag. The drag shows up as late notes, coder queries, unclear medical necessity, and inbox floods. Many teams try to solve this with “work harder” tactics, but the real problem is the system. Remote scribing shifts documentation from an after hours task into a live workflow, which is why it directly supports the documentation shifts highlighted in 2025 healthcare documentation trends.
The second reason remote scribing is accelerating is telehealth. Telehealth visits can be short, but the documentation still has to be complete, consistent, and defensible. In reality, telehealth often creates heavier edits because providers defer charting until later. Remote scribes remove that backlog by structuring the note during the call. If your organization is already feeling this pressure, the patterns in rising demand for scribes in telehealth and the directory of telehealth companies using medical scribes make it clear this model is becoming standard.
Remote scribing also solves a staffing reality. Many organizations cannot hire locally at the speed they need. Remote coverage opens a wider talent pool and supports flexible scheduling without breaking continuity. That matters for high volume settings that need reliability, such as the environments featured in emergency departments and urgent care chains and systems hiring at scale in the health systems by state mega list.
The final driver is compliance. Documentation expectations keep tightening, and inconsistent notes create audit risk. Remote scribing helps standardize templates, enforce phrasing patterns, and reduce missing elements. If you want the compliance angle framed correctly, use navigating new compliance and documentation standards and documentation compliance requirements as the foundation for how you train and monitor quality.
| Capability | Primary Outcome | Target KPI | Proof Artifact |
|---|---|---|---|
| Standard note templates Consistency |
Less rework | Template adherence ≥ 95% | QA sampling report |
| Macro and phrase library Speed |
Faster documentation | Macro reuse ≥ 70% | Macro analytics export |
| Remote access protocol Security |
Lower risk | 0 policy exceptions | Access audit log |
| Audio quality standards Reliability |
Fewer missed details | Audio issue rate under 3% | Incident tracker |
| Visit agenda preloading Preparedness |
Shorter start delays | Late starts down 20% | Schedule variance |
| Med list reconciliation support Safety |
Cleaner charts | Reconcile completion ≥ 98% | Chart completeness audit |
| Problem list hygiene Clarity |
Fewer coder queries | Duplicate problems down 30% | Problem list QA |
| Medical necessity phrasing prompts Defensibility |
Fewer denials | Doc related denials down 15% | Denial reason trend |
| Same day sign off standard Backlog kill |
Less after hours work | Same day sign off ≥ 90% | EHR timing export |
| Order entry support rules Flow |
Fewer delays | Order completion lag down 20% | Order timing snapshot |
| Referral packet checklist Closure |
Cleaner referrals | Referral bounce backs down 25% | Referral log |
| Telehealth documentation kit Edit reduction |
Less provider editing | Edits per note down 30% | QA comparison sample |
| Specialty specific templates Precision |
Better coding clarity | Specific ICD use ≥ 95% | Coder QA sample |
| Structured ROS blocks Completeness |
Fewer missing elements | ROS completion ≥ 98% | Completeness audit |
| Exam capture standards Accuracy |
Cleaner documentation | Exam errors under 2% | QA scorecards |
| Medical decision making structure Trust |
Less clarification needed | Coder queries down 20% | Query log trend |
| Escalation path for clinical questions Speed |
Fewer stalled notes | Escalations resolved under 10 min | Escalation tracker |
| Provider preference profiles Adoption |
Lower friction | Ramp time under 14 days | Onboarding checklist |
| Shift handoff checklist Continuity |
Fewer dropped tasks | Handoff misses under 2% | Handoff audit |
| Downtime fallback workflow Resilience |
Stable operations | 0 missed notes | Downtime incident log |
| Documentation version control Audit readiness |
Faster audits | All templates tagged | Version index |
| Secure communication channel Clarity |
Fewer interruptions | Message volume down 15% | Messaging analytics |
| Daily QA sampling Quality |
Cleaner first pass notes | QA score ≥ 95% | QA dashboard |
| Weekly coaching loop Improvement |
Fewer repeat errors | Top error rate down 25% | Coaching notes |
| Metric reporting cadence Proof |
Faster leadership buy in | Reports delivered weekly | Ops scorecard |
| Billing and coding feedback loop Revenue |
Fewer denials | Downcodes down 10% | Downcode report |
| Coverage model across time zones Capacity |
More availability | Coverage gaps under 2% | Coverage calendar |
| Patient privacy environment checks Safety |
Lower privacy risk | 100% compliance | Attestation log |
2) How Remote Scribing Actually Changes the Documentation Workflow
Remote scribing works when it is treated like a production line, not a helper role. The goal is a consistent flow from visit start to signed note, with fewer interruptions and fewer edits. This is the same operational logic behind the performance gains discussed in medical scribe efficiency innovations, but remote adds two extra requirements: communication clarity and security discipline.
Before the visit, remote scribes remove context switching. They can preload the note skeleton, review prior notes, pull recent labs, and set up a focused plan section so the provider does not start from a blank page. When this step is missing, providers spend the first minutes searching, then forget key history details, then add addenda later. If you want a model for structured prep, combine templates with systems from the office management software directory for CMAAs and stable storage from document management tools for medical administration.
During the visit, the remote scribe protects the clinician’s attention. Remote scribing is at its best when the provider stays in conversation, while the scribe captures HPI, ROS, exam elements, and the plan structure in real time. That reduces the cognitive load that leads to missed details and repeated questions later. It also improves the continuity of care because the note tells a clear story, which aligns with the coordination gains described in how medical scribes improve patient care coordination.
After the visit, remote scribing kills chart debt. Most clinics do not realize how much operational drag comes from notes sitting unsigned. When notes are delayed, coding slows down, billing slows down, follow up tasks become unclear, and compliance risk rises. A remote workflow that targets same day sign off creates a measurable impact on revenue and staff workload. If you need proof focused language for stakeholders, use the framing from the real time industry report on data accuracy and anchor it to the compliance pressure described in medical scribes and documentation compliance.
Remote also unlocks scalability. A remote pool can cover multiple providers, multiple sites, and extended hours without depending on local hiring. That matters in competitive markets where programs struggle to staff reliably. You can see how scale is already shaping demand by comparing the physician groups and MSOs hiring scribes and the broader footprint in the health systems hiring by state.
3) Compliance, Security, and Quality in Remote Scribing
Remote scribing succeeds or fails on trust. Leaders worry about privacy, access control, and note quality. Providers worry about accuracy and workflow friction. Coders worry about incomplete medical decision making. If you build the program around these fears, adoption becomes smoother and the value shows up faster. The easiest way to do that is to treat compliance and quality as design requirements, not training afterthoughts.
Start with documentation standards. Remote scribes must know how to structure notes so they read cleanly and defensibly. That includes capturing decision making, documenting medical necessity, and avoiding vague phrasing that triggers coder queries. If your organization is updating standards, use navigating compliance and documentation standards as the baseline and reinforce it with documentation compliance guidance.
Then lock down the workflow. Remote scribing should have a defined access method, a consistent communication channel, and a documented escalation path for clinical questions. If those are missing, remote scribes will improvise, and improvisation is where risk grows. For communication, align tools with the medical office communication tools directory. For coordination, build task ownership with the systems in the task management software guide for CMAAs.
Quality is the other pillar. A remote program needs ongoing QA because distance increases the chance of small misunderstandings. That does not mean micromanagement. It means sampling, scoring, and coaching. A simple loop works: sample daily, coach weekly, and publish monthly metrics. When you do that, providers sign notes faster because they trust the output. It also keeps your program aligned with the evolving environment described in healthcare documentation trends.
Finally, choose tech that reduces edits, not creates cleanup. Many teams chase shiny tools, then realize they added another layer of work. When you evaluate assistive tools, focus on how much they reduce editing burden and whether they support consistent structure. Cross reference voice recognition and dictation software with the market view in AI and ambient scribe tools to avoid buying tech that forces your team to rewrite everything anyway.
4) Implementation Blueprint for Remote Medical Scribing That Actually Sticks
A remote program should be implemented like an operations rollout, not a hiring experiment. The clinics that win start small, standardize fast, and measure everything. The clinics that struggle try to go wide immediately, then spend months patching exceptions.
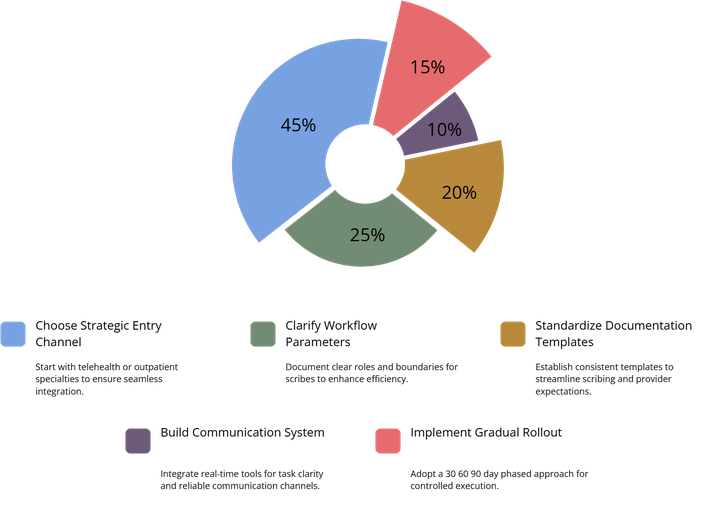
First, choose the right starting lane. Telehealth is often the cleanest entry point because the visit already runs through a digital channel. High volume outpatient specialties are another strong starting lane because documentation burden is high and templates can be standardized. If you want to see where demand is concentrated, compare hiring patterns in outpatient specialty networks and the broader growth picture in national medical scribe hiring surge.
Second, define the workflow boundary in writing. Remote scribing breaks when the role is fuzzy. Document what the scribe captures, what the provider verifies, and what the scribe is not allowed to do. Pair that boundary with template standards so providers know what to expect. This is where a program becomes scalable rather than personal. For baseline expectations, align training with medical scribe careers with certification and reinforce skill development using the training courses and certifications directory.
Third, build the tool chain that protects speed. Remote scribes need reliable communication and task ownership. If the scribe has to guess whether a lab follow up is needed, that turns into a message, then an interruption, then a delay. Instead, build a system where tasks are created, assigned, and closed with clear ownership. Use the structure suggested by workflow automation tools for medical admin and the practical systems in task management software for CMAAs.
Fourth, run a 30 60 90 day rollout with measurable milestones.
In the first 30 days, focus on one provider group, one template set, one QA scorecard, and a daily sign off standard. In the next 30 days, expand coverage hours and tighten macro libraries. In the final 30 days, add a billing feedback loop so coding and denials improve over time. Tie the rollout to real metrics, similar to the operational lens used in medical administration workforce trends and use compliance framing from documentation compliance standards.
5) The Results That Matter: Efficiency, Revenue, and Provider Experience
Remote scribing should not be sold as “typing help.” It should be sold as measurable operational performance. The core outcomes to track are speed, quality, and downstream rework. When all three improve together, you have real transformation.
Efficiency metrics that show the day is getting lighter. Track percent of notes signed same day, average time from visit end to sign off, and after hours charting minutes. These indicators expose chart debt. Chart debt is the root cause of burnout and sloppy follow up. If your organization needs a stronger narrative for leadership, connect results to the trends described in healthcare documentation trends and the performance focus in medical scribe efficiency innovations.
Quality metrics that protect compliance and coding. Track coder query volume, downcoding trends, denial reasons tied to documentation, and audit findings. Remote scribing improves these metrics when templates are standardized and medical decision making is captured cleanly. If you want a strong quality reference point, align with data accuracy reporting and link it to documentation compliance guidance.
Revenue cycle metrics that prove this is not a soft benefit. Faster sign off supports faster coding and fewer claim holds. Better documentation supports cleaner first pass claims. Remote scribing can reduce rework for billing teams, which is often overlooked when leaders focus only on provider time. If your organization is dealing with payer friction, pairing remote scribing with standardized admin workflows from the best office management software directory and stable storage from document management tools makes the operational gain stick.
Provider experience metrics that predict retention. Measure provider satisfaction and turnover risk indicators. Remote scribing helps providers leave on time, reduce late night charting, and stay present with patients. The clinics that quantify this see it as a retention tool, not only a productivity tool. If your workforce planning includes location strategy, map staffing availability using best cities for medical scribe careers and hiring patterns in health systems by state.
6) FAQs: Remote Medical Scribing and Documentation Transformation
-
They treat it like a staffing swap instead of a workflow redesign. Without standardized templates and a clear boundary of responsibility, remote scribes spend weeks adapting to personal habits, which slows adoption and increases edits. The fix is simple: one core template set, one macro library, and one QA scorecard that defines quality. Use medical scribe efficiency innovations to frame the workflow improvements and anchor compliance to documentation standards so speed never becomes risk.
-
It works for both, but the workflow is different. Telehealth is naturally compatible because the visit already happens through a digital channel, which reduces setup friction. In person workflows need reliable audio capture and a stable communication path to resolve clarifications quickly. Many programs start in telehealth, prove results, then expand. The adoption curve described in telehealth scribe demand and the market footprint in the telehealth company directory show why this approach is common.
-
Track coder query volume, addenda rates, and QA sampling scores against a defined checklist. Quality is not a feeling. It is a repeatable standard. The strongest programs publish a monthly dashboard with completeness, accuracy, and compliance alignment. Use the structure from real time data accuracy reporting and connect it to compliance and documentation standards so leadership sees both performance and risk control in one view.
-
They need medical terminology, documentation structure, specialty context, privacy discipline, and strong template literacy. Then they need clinic specific training on your note formats, macros, escalation paths, and QA standards. This is why programs with a clear pipeline scale faster. If you want a clean training reference, use medical scribe careers with certification and the directory of scribe training courses to standardize expectations across hires.
-
AI can help, but only when your templates and QA system are already disciplined. Draft generation is not the same as compliant, structured documentation. Many clinics use AI to accelerate capture, then rely on scribes to ensure structure, accuracy, and medical necessity phrasing. If you evaluate tools, focus on edit burden and workflow fit, not feature lists. Compare the landscape in AI and ambient scribe tools and the more traditional approach in dictation software before you commit.
-
They improve revenue cycle performance by reducing late notes, capturing cleaner medical decision making, and lowering coder queries that delay billing. Cleaner documentation also reduces denials tied to missing medical necessity or unclear plans. The value becomes visible when you track first pass claim quality alongside sign off speed. To align admin workflows around this, connect operations to the systems in workflow automation tools for medical admin and the control needed for audits described in documentation compliance guidance.
-
Adoption is strongest where documentation burden and volume pressure are high: telehealth, urgent care, ED, and busy specialty networks. These environments feel the cost of chart debt immediately, so leadership prioritizes solutions that reduce after hours work and improve throughput. If you want a market view, compare the employer footprint in health systems hiring by state with high volume environments in the urgent care and ED directory and specialty demand in outpatient networks hiring scribes.