

Patient Flow Management Terms: Interactive Guide & Scenarios
In modern healthcare systems, patient flow management is not just a background operation—it is the operational spine of every successful facility. From emergency departments to long-term care wings, the ability to track, route, and discharge patients efficiently determines everything from patient safety to provider burnout. When flow breaks down, so does care delivery. Bottlenecks increase length of stay (LOS), delay diagnostics, and create ripple effects across departments that compromise quality outcomes.
Yet most disruptions stem not from technology gaps, but from terminology confusion and poor protocol standardization. When nurses, scribes, and administrators use inconsistent language—especially in moments of crisis—handoffs become error-prone, transfers stall, and patients get stuck in limbo. That’s why mastering the core patient flow vocabulary isn’t academic—it’s critical. This guide breaks down high-impact terms and shows how they're used in real scenarios to cut chaos, accelerate decision-making, and build a safer, more responsive clinical environment.

Core Concepts in Patient Flow
Admission to Discharge Pipeline
Patient flow begins well before the hospital doors open and ends long after a discharge summary is printed. This entire pipeline—from pre-admission through discharge—is a complex, time-sensitive choreography involving multiple departments, systems, and roles. Understanding this flow is the foundation of operational readiness.
Pre-admission & Intake
Pre-admission planning involves triage-level decisions based on acuity, insurance verification, and anticipated care needs. Intake isn’t just about collecting data; it initiates clinical prioritization and sets throughput expectations. Delays at this stage create downstream ripple effects—especially in high-volume EDs—leading to unnecessary transfers, missed diagnostics, or prolonged wait times.
Smart intake systems now integrate predictive modeling to flag patients likely to escalate in care needs, ensuring that bed assignments and diagnostics align with clinical urgency. This also improves capacity forecasts and keeps unnecessary admits out of observation units.
Bed Assignment Logic
Assigning beds isn’t a clerical task—it’s a clinical and operational decision. Factors include isolation precautions, acuity level, specialty match, and gender mix. Poor bed logic results in overuse of telemetry, misuse of ICU resources, or patients stuck in hallways.
Centralized bed boards powered by real-time location data or AI-driven scoring reduce manual errors and enhance speed. Understanding how terms like blocked bed, ready bed, and bed hold function in context helps eliminate inefficiencies and boosts turnover rates across med-surg and step-down units.
Throughput Optimization
Optimizing throughput is about minimizing delays between clinical milestones—triage, diagnostics, consults, transfers, and discharge. Every hour saved reduces LOS, infection risk, and ED congestion.
Transfer Delays & LOS Metrics
Transfer delays are often caused by coordination failures between departments. Miscommunications on order entry timing, incomplete documentation, or pending labs stall transfers. By closely monitoring LOS metrics broken down by unit and service line, hospitals gain visibility into where delays cluster and which roles need accountability.
Common key performance indicators (KPIs) include:
Decision-to-admit time
Time to bed assignment
Discharge order to patient departure
Reducing each of these by even 15 minutes has measurable impacts on daily census balance and clinical capacity.
Discharge Planning Signals
Discharge planning begins on admission. Yet many facilities still treat it as a late-game step. Early identification of barriers—social work consults, pending tests, transportation—allows staff to avoid last-minute delays.
Modern discharge tools track signals like:
Projected discharge date (PDD)
Discharge readiness score
Disposition match (home, SNF, rehab)
By aligning these with clinical progress notes and case management flags, teams can free beds earlier, reduce patient frustration, and maintain smoother morning discharges—when most admissions spike.
| Component | Description | Impact on Patient Flow |
|---|---|---|
| Pre-admission & Intake | Early triage, insurance checks, predictive risk modeling | Aligns diagnostics and bed use with acuity, prevents bottlenecks |
| Bed Assignment Logic | Bed placement based on isolation, acuity, gender, specialty; uses centralized bed boards | Reduces hallway boarding, ICU misuse, and delayed transfers |
| Throughput Optimization | Minimizing time between care milestones (e.g., triage, consults, transfers, discharge) | Cuts LOS, boosts ED capacity, improves safety |
| Transfer Delays & LOS | Time lost due to miscommunication or documentation gaps between units | LOS metrics highlight problem areas and drive accountability |
| Key LOS KPIs | Decision-to-admit time, time to bed assignment, discharge order to patient departure | Each 15-min gain improves census balance and clinical efficiency |
| Discharge Planning Signals | Tools and metrics: Projected discharge date (PDD), readiness score, disposition match | Enables early bed release, faster admissions, and improved satisfaction |
Common Patient Flow Terms Explained
Queue Management
Queue management refers to how patients are sequenced through different phases of care—triage, diagnostics, consultation, and admission. It’s not just about who waits longer, but why they’re waiting and how resources are dynamically reallocated. A hospital that manages its queues well can adapt to shifting volumes, acuity surges, and staffing shortages in real time.
Scenario: At 9:15 a.m., the ED hits capacity. A patient with moderate abdominal pain is queued behind two higher-acuity cases. Real-time queue dashboards alert charge nurses, who reassign available physicians based on average wait time thresholds. The result? The lower-acuity patient is seen within the 30-minute window, keeping throughput intact and satisfaction high.
Diversion Status
Diversion is a formal declaration that the hospital or specific units cannot safely accept more patients. This may include ED diversion, trauma diversion, or cath lab closure. These statuses signal to EMS and transfer coordinators to reroute incoming patients.
Scenario: A Level 1 trauma center experiences a simultaneous code blue and two ICU discharges pending. Without timely updates, EMS continues to route unstable patients. By activating trauma diversion status and alerting the regional hub, avoidable delays and patient safety risks are minimized.
Boarding
Boarding occurs when admitted patients remain in the ED due to unavailable inpatient beds. It’s one of the biggest bottlenecks in flow, often leading to increased LOS, staff burnout, and safety events.
Scenario: Three admitted patients are boarded in the ED hallway. One is diabetic with unstable glucose, and another is pending psych evaluation. By clearly labeling these patients in the EHR with ED boarding status and escalating to bed control, inpatient charge nurses reprioritize discharges, opening capacity by noon. Clear boarding terminology enabled rapid mobilization.
ED Throughput
ED throughput measures how efficiently patients move through the emergency department—from door to provider, provider to disposition, and disposition to exit. Each delay adds risk, lowers satisfaction, and strains adjacent units.
Scenario: Door-to-provider time exceeds 45 minutes for non-urgent cases. Reviewing throughput analytics, it’s found that labs are delayed by 12 minutes due to sample batching. Micro-adjusting phlebotomy dispatch and shifting to rolling lab runs reduces turnaround time, improving total throughput.
Capacity Alerts
Capacity alerts are system-wide flags based on internal thresholds—typically triggered by a combination of census levels, pending discharges, and staff availability. Unlike diversions, capacity alerts may not change external routing but force internal escalation protocols.
Scenario: A med-surg unit hits 95% occupancy with five patients awaiting step-down beds. A capacity alert triggers auto-notifications to case managers, activates the early discharge team, and freezes elective admissions. These alerts prevent passive overflow and coordinate rapid decompression.
| Term | Definition | Scenario Summary | Operational Impact |
|---|---|---|---|
| Queue Management | Organizing patient sequencing across care phases using real-time adjustments | Lower-acuity patient seen quickly after real-time dashboard triggers physician reassignment | Maintains throughput and reduces wait-time dissatisfaction |
| Diversion Status | Official notification that hospital/unit cannot accept more patients | Trauma diversion activated during simultaneous critical events to reroute EMS traffic | Minimizes patient risk and avoids overload in critical areas |
| Boarding | Holding admitted patients in ED due to lack of inpatient beds | ED hallway patients labeled as ‘boarded’ and escalated to inpatient charge nurses for bed reprioritization | Frees up space faster and prevents safety issues |
| ED Throughput | Speed of patient progression through ED steps (arrival to exit) | Sample batching delays lab results; switched to rolling dispatch to improve flow | Reduces LOS and improves efficiency across diagnostics and care |
| Capacity Alerts | Internal triggers signaling overload based on census, staff, discharge metrics | 95% occupancy triggers alert; early discharges prioritized and elective admissions frozen | Prevents overflow and triggers coordinated escalation |
Scenario-Based Learning: Term Applications in Real Settings
Case Study 1 – Emergency Room Overflow
At 3:00 p.m., an urban trauma hospital receives a multi-vehicle crash alert. Within minutes, the ED swells with twelve new arrivals. Simultaneously, five patients from earlier in the day remain boarded due to unavailable inpatient beds. The charge nurse activates a capacity alert and pushes a real-time ED throughput report to the operations team.
Bed control initiates a “bed sweep,” updating occupancy by unit. Triage nurses assign diversion status for minor cases, rerouting them to urgent care. Meanwhile, a command center liaison triggers a predefined protocol: early discharge reviews, psych hold escalations, and portable imaging for patients stuck in overflow zones. The result? Room is created for two high-acuity trauma cases in under 40 minutes—avoiding EMS reroute and mitigating risk.
Case Study 2 – ICU Bed Turnaround
A 64-year-old post-op cardiac patient stabilizes overnight and is marked for transfer to a step-down unit by 7:00 a.m. However, bed assignment delays stretch the transfer past 10:00 a.m. A review reveals that discharge orders in the receiving unit were entered late and two “ready beds” had not been cleared in the EHR.
The incident triggers a LOS audit and a transfer delay tag is added to the daily throughput dashboard. By standardizing bed readiness signals, revising case manager rounding times, and using predictive analytics to forecast ICU step-down demand, the hospital reduces average ICU turnaround from 5.4 to 3.1 hours.
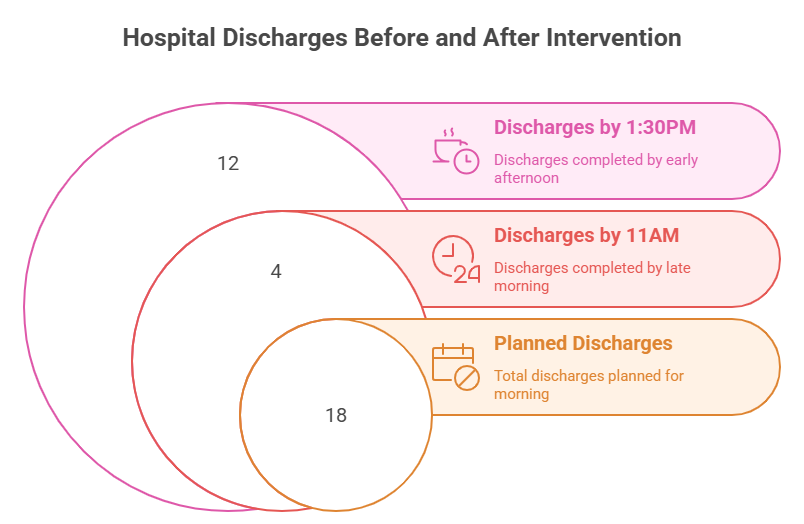
Case Study 3 – Discharge Backlog Impact
On a Monday morning, 18 patients are scheduled for discharge. By 11:00 a.m., only four have left the building. The hold-up? Delays in transportation coordination, final labs, and consult notes. Patients slated for morning discharge are occupying beds needed by noon admits from the ED.
A nurse flags the discharge status as “pending non-clinical delay.” This term routes the issue to the discharge facilitation team, triggering a cascade: social work prioritization, courier engagement for take-home meds, and attending escalations for pending notes. By 1:30 p.m., 12 patients are discharged, freeing capacity for seven incoming ED admits and preventing an ED boarding spike.
Digital Tools for Patient Flow
Real-Time Location Systems (RTLS)
RTLS technology tracks the real-time movement of patients, staff, and equipment within the facility using RFID or Bluetooth tags. This visibility enables instant alerts when bottlenecks form, such as a patient waiting too long in radiology or a stretcher left in the hallway. More importantly, RTLS supports dynamic bed turnover by alerting environmental services (EVS) the moment a patient is discharged.
When integrated with capacity management platforms, RTLS drives actionable metrics like:
Time to room assignment
EVS response time
Diagnostic turnaround tracking
By using these systems, teams can cut room idle time by 20–40%, shaving hours off average LOS and improving throughput across departments.
EHR-Integrated Dashboards
Modern EHRs offer more than patient charts—they include dashboards that consolidate real-time flow metrics. These dashboards pull from multiple data points: census, discharge orders, radiology results, consult completions, and more.
High-functioning dashboards allow clinical and operational leads to:
Prioritize pending discharges
View ED-to-floor delay trends
Monitor boarding volume by hour
These insights help charge nurses and bed managers make rapid, data-driven decisions, rather than relying on fragmented verbal updates or outdated spreadsheets.
Predictive Analytics for LOS Forecasting
AI-driven tools now predict patient length of stay based on historical patterns, comorbidities, diagnostics, and even social determinants of health. These forecasts help case managers and clinicians make proactive discharge plans and allocate resources with precision.
Examples include:
Identifying patients at risk for long LOS before admission
Flagging missing care milestones that delay transitions
Modeling how one delayed discharge could impact next-day census
Hospitals using predictive LOS models report up to 30% faster discharge execution and a significant drop in ED boarding during peak hours. These models also integrate with financial planning by aligning staff allocation with projected volume—turning patient flow into a strategic lever.

Common Mistakes in Using These Terms
Mislabeling Bottlenecks
One of the most damaging errors in patient flow management is misidentifying the true cause of a delay. Teams often label a slow discharge as a “transport issue” when the real problem was a delayed discharge order or pending lab result. Mislabeling leads to misdirected interventions—slowing improvement and creating unnecessary friction between departments.
For instance, when case managers tag all delays as disposition pending, it hides operational gaps in provider rounding or pharmacy turnaround. Precision in bottleneck terminology isn't semantics—it's the foundation for targeted flow acceleration.
Confusing Triage Tags with Priority Codes
Triage tags and priority codes are not interchangeable. Triage tags (e.g., red, yellow, green) are used to categorize clinical urgency during mass casualty or ED intake, while priority codes (e.g., Priority 1, 2, 3) guide transport sequencing or internal escalations.
When clinicians or scribes mix these up in EHR documentation, it can lead to misrouted patients, delayed imaging, or even inappropriate admissions. Clear training on their use ensures smoother transitions and accurate analytics across emergency and inpatient care.
Misuse of ED-to-Floor Delay Terminology
Terms like ED delay, bed delay, and admission hold are often used interchangeably—but they shouldn’t be. Each one indicates a different problem. ED delay typically reflects clinical factors—labs, imaging, or consults. Bed delay signals logistical or space issues, while admission hold often results from documentation or insurance processing lags.
Incorrect labeling in throughput dashboards skews data interpretation. Leadership might allocate more staff to EVS when the real issue is unfinalized discharge summaries upstream. By tightening terminology usage, teams gain clarity in root cause analysis and unlock more precise workflow fixes.
| Mistake | Description | Consequence | Corrective Action |
|---|---|---|---|
| Mislabeling Bottlenecks | Incorrectly identifying the source of delays (e.g., blaming transport instead of late discharge orders) | Misdirected solutions, delayed throughput improvements, departmental tension | Train teams to use accurate delay categories aligned with root causes |
| Confusing Triage Tags with Priority Codes | Mixing up ED triage tags (urgency) with transport or escalation codes (priority) | Patient misrouting, delayed diagnostics, admission errors | Standardize training on tag/code definitions for EHR accuracy and handoff clarity |
| Misuse of ED-to-Floor Delay Terminology | Using ED delay, bed delay, and admission hold interchangeably without understanding distinctions | Skewed dashboard analytics, misguided resource allocation | Clarify definitions and enforce proper use in documentation and analytics |
How ACMSO Trains Scribes to Master Patient Flow—Not Just Document It
Patient flow terminology isn’t just for administrators—medical scribes are on the frontline of clinical documentation, and their accuracy shapes how patient movement is interpreted. The Medical Scribe Certification by ACMSO trains students not only in medical terminology but in the real-world language of hospital operations, throughput, and discharge efficiency.
Scribes trained under this certification learn to:
Document boarding status and ED-to-floor delays with operational accuracy
Tag admission types (e.g., direct admit, observation, elective surgery)
Capture provider-stated discharge barriers or disposition shifts in live charting
Use structured language that supports EHR-integrated dashboards
Through ACMSO’s 12-module training system, scribes practice with simulated EHR templates, encounter note protocols, and interdisciplinary workflows. These lessons directly align with hospital terms like:
Disposition pending due to social clearance
Admit hold for MRI completion
LOS extended due to specialty consult backlog
This precision turns documentation from passive recordkeeping into a strategic asset that improves patient flow.
The certification also covers compliance fundamentals like HIPAA, time-stamping, and chain-of-command escalation—all of which influence how quickly bottlenecks are resolved or escalated.
Graduates of the program are equipped to step into fast-paced hospital units, urgent care centers, or telehealth hubs and immediately contribute to operational clarity. In clinical settings where every delay can ripple across departments, this kind of trained documentation can reduce noise, guide leadership decisions, and accelerate patient throughput at scale.
Frequently Asked Questions
-
Patient flow management refers to the coordinated movement of patients through different stages of care—from arrival to discharge. It involves optimizing how patients are admitted, transferred, and discharged to avoid delays, reduce overcrowding, and enhance resource use. Effective flow management depends on real-time communication, smart bed assignment, discharge planning, and data-informed decision-making. When executed well, it can lower length of stay (LOS), improve patient satisfaction, and boost clinical outcomes. It’s not just a logistical concern—it’s a clinical priority for safety and operational sustainability.
-
Inconsistent use of terminology causes breakdowns in coordination. When staff use vague or overlapping terms—like saying “delay” without specifying admission delay vs. bed delay—the result is misaligned handoffs and flawed performance analytics. Standardizing terms like boarding, diversion status, and LOS across EHR systems and teams ensures everyone responds with clarity and urgency. Standardized language improves escalation accuracy, enables automation, and helps identify true bottlenecks, leading to measurable improvements in throughput and discharge efficiency.
-
Boarding happens when admitted patients stay in the emergency department (ED) due to a lack of available inpatient beds. Common causes include slow discharge processes, late provider rounding, and documentation delays. To resolve boarding, hospitals must align discharge and admission workflows, use real-time bed dashboards, and implement early discharge protocols. Additional strategies include pre-admission screening, centralized bed management teams, and predictive models to anticipate bottlenecks. Reducing boarding not only improves patient flow—it also mitigates safety risks and reduces staff fatigue.
-
Predictive analytics use historical and real-time data to forecast patient needs and system capacity. In patient flow, these tools anticipate discharge readiness, identify likely delays in diagnostics, and even suggest alternative care pathways. They support LOS forecasting, helping teams proactively plan for bottlenecks before they occur. By flagging high-risk cases early, analytics improve prioritization and resource allocation. Hospitals using predictive tools have reported lower LOS, reduced ED boarding, and fewer preventable escalations, making analytics a strategic advantage in clinical operations.
-
Diversion status is a formal notice to EMS and transfer systems that a unit or hospital cannot accept new patients due to capacity or resource limits—redirecting traffic externally. A capacity alert, on the other hand, is an internal escalation that signals critical strain within the hospital. It does not stop incoming traffic but prompts immediate internal actions: early discharge acceleration, elective surgery review, or staff redeployment. Both tools are vital, but they serve different purposes—diversion controls volume inflow, while capacity alerts mobilize internal response.
-
The most used patient flow metrics include:
Length of Stay (LOS)
Door-to-provider time
ED boarding hours
Discharge order-to-departure time
Transfer delay time
Each metric captures a different phase of the flow process. LOS measures the total time a patient spends in the facility, while boarding time highlights gaps between admission and bed availability. Accurate tracking of these KPIs allows teams to identify bottlenecks, set performance benchmarks, and implement targeted improvements that enhance throughput and capacity planning.
-
Medical scribes play a key role in accurate, real-time documentation of events that influence patient flow—such as delays, bed assignments, and discharge notes. Scribes trained through the Medical Scribe Certification by ACMSO are taught to use precise terminology that aligns with operational protocols. Their documentation helps providers spend more time on clinical care while supporting throughput tracking and analytics. Scribes also assist with discharge summaries, consult tracking, and escalation notes—reducing administrative delays and improving team coordination.
Final Thoughts
Every minute a patient waits in the wrong place is a minute of lost safety, efficiency, and resource alignment. Patient flow is not just a logistics function—it’s a clinical imperative. From ED boarding to ICU turnaround, the terms and tools described in this guide offer a shared language for real-time problem solving.
When clinicians, scribes, and operations teams speak in precise, aligned terminology, they unlock faster decisions, reduce rework, and prevent cascading delays. Learning these terms in isolation isn't enough—what matters is applying them in live scenarios, tied to dashboards, automation tools, and escalation protocols that protect patient outcomes.
Whether you’re documenting a discharge barrier or escalating a capacity alert, your words carry weight. Master the vocabulary, master the system.
| Which patient flow term do you think is most misunderstood in real-world hospital settings? |
| 1. ED Boarding |
| 2. Diversion Status |
| 3. Capacity Alert |