

Denial Management: Practical Solutions for Medical Admin Assistants
Denials rarely begin in the billing office. They usually begin earlier, during patient intake, weak insurance verification, sloppy appointment scheduling, incomplete front-desk operations, or poor patient communication. That is why denial management belongs on every strong medical admin assistant’s skill list.
This guide explains how medical admin assistants can prevent avoidable denials, support cleaner claims, document smarter in the EMR, communicate clearly with patients, and build the kind of operational reliability that strengthens career growth, improves healthcare efficiency, and makes them far more valuable to any practice.

1. Why Denial Management Starts Long Before the Claim Is Rejected
A denial feels like a back-end event because it shows up after the visit, after documentation, and after the claim goes out. In reality, most denials are planted upstream by registration mistakes, missing coverage details, bad referral handling, weak authorization tracking, incomplete chart updates, and appointment setups that never matched payer rules in the first place. That is why medical admin assistants who understand medical billing terms, insurance verification workflows, scheduling conflicts, patient intake procedures, and front-desk operations prevent far more revenue damage than people realize.
This matters because a denial is never just a financial inconvenience. It creates rework, delays statements, frustrates patients, increases staff follow-up, weakens provider confidence in office operations, and often exposes where the team is guessing instead of using reliable workflows. A wrong subscriber ID, old payer on file, missed referral, or unsupported visit type can force multiple departments to spend time cleaning up one preventable error. That is why denial management connects directly to patient communication apps, healthcare CRM terms, EMR and charting terms, patient privacy communication essentials, and medical records release tools. Good denial work protects both revenue and trust.
The strongest medical admin assistants understand that denial prevention is a systems skill. They do not wait for a rejection code to tell them something went wrong. They look for risk before the visit even starts. They ask whether the patient is booked correctly, whether the insurance on file is still active, whether the referral belongs to the right provider, whether prior authorization is needed, whether the chart reflects the right demographics, and whether the patient understands what documents or payments are expected before arrival. That mindset grows from studying secure patient scheduling tools, medical office automation trends, the future of EMR systems, future compliance changes for CMAAs, and data privacy guidance. Denial management is operational discipline wearing a financial consequence.
2. The Denial Categories Medical Admin Assistants Can Influence Most
The easiest mistake is assuming denials belong only to coders or billers. Medical admin assistants influence the denial categories that happen most often in everyday practice: eligibility, demographic accuracy, referral status, authorization status, scheduling fit, consent completion, documentation routing, and patient communication gaps. Those areas sit directly inside appointment scheduling workflows, patient intake checklists, insurance verification processes, EMR integration tools, and front-desk operations systems. If those are weak, the claim starts its life already damaged.
Eligibility denials often happen because staff verify too early and never recheck close to the date of service. Patients change jobs, plans terminate, subscriber relationships shift, and secondary payers appear without warning. A practice that books four weeks out and never reconfirms insurance is practically inviting preventable denials. That is why strong teams use secure scheduling tools, patient communication apps, healthcare portals, medical admin staff scheduling tools, and medical admin time-tracking tools to create timing discipline around re-verification.
Referral and authorization denials usually expose a process gap rather than a knowledge gap. Staff often know those items matter. The real problem is that nobody owns the trigger, nobody tracks the due date, and nobody confirms that the authorization actually matches the visit, the provider, the place of service, and the date. That is where collaboration tools for medical office teams, patient communication workflows, healthcare CRM terms, medical records release tools, and telehealth platform knowledge become denial-prevention assets, not just nice-to-have tools.
Demographic and communication-related denials are quieter and more dangerous because people dismiss them as small registration errors. A wrong birth date, missing middle initial, outdated address, incorrect guarantor, incomplete policy holder relationship, or bad phone number can derail clean claims, delay patient outreach, and weaken appeals later because the paper trail is inconsistent. That is why medical admin assistants should understand HIPAA and patient privacy terms, patient privacy communication essentials, active listening techniques, difficult patient conversation management, and de-escalation techniques. Denials often shrink when conversations get sharper.
3. A Practical Denial Workflow From First Alert to Last Follow-Up
When a denial lands, the first move is classification. Do not jump straight into action before understanding exactly what failed. Was this an eligibility denial, demographic mismatch, authorization issue, referral issue, documentation gap, payer edit, or scheduling setup problem? Medical admin assistants who work denials well pair the denial reason with what happened at the front end: how the patient was booked, what insurance was captured, what communication took place, what documents were attached, and whether the EMR and portal workflow reflected the same story. That is where knowledge of medical billing terms, EMR charting terms, patient intake definitions, and front-desk workflow language pays off.
The second move is source tracing. Find the earliest point where the error entered the workflow. Did the patient give updated insurance and nobody saved it? Did the scheduler book the wrong visit type? Was the referral scanned but never routed? Did the patient portal contain a message that staff never acted on? Did the patient receive weak instructions and arrive with incomplete paperwork? This kind of tracing improves when teams use patient communication apps, medical office collaboration tools, records release workflows, healthcare CRM systems, and medical office automation tools. The goal is not to blame the first person who touched the chart. The goal is to find the step that failed.
The third move is correction with visibility. Once the problem is known, fix the affected data in the right place, attach the right support, route the issue to the correct person, and make the next action obvious. Vague notes kill denial workflows. Clear notes move them. A strong denial note identifies what was wrong, what was corrected, what proof supports the correction, what date the correction happened, and what follow-up remains. That discipline depends on patient privacy rules, HIPAA terminology, effective patient communication, healthcare portal literacy, and EMR update discipline. Clean follow-up is how denials stop aging into write-offs.
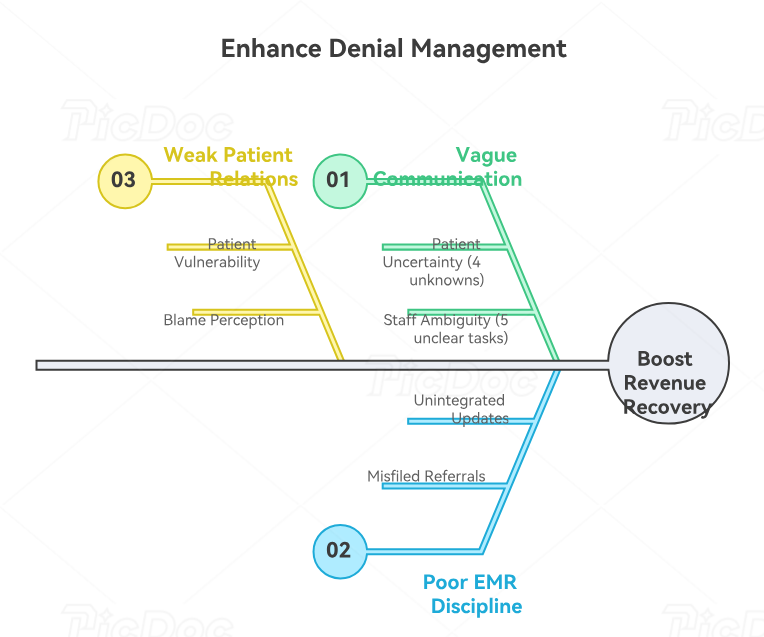
4. Communication and EMR Habits That Cut Repeat Denials
Denial management gets weaker when communication stays vague. Patients hear “there was an issue with your insurance” and still do not know what to send, where to send it, how urgent it is, or what happens next. Staff hear “fix the denial” and still do not know whether the right task is getting a new card, confirming active coverage, obtaining a referral, updating a guarantor, or attaching outside documentation. Strong medical admin assistants solve this by using precise language, documented next steps, and consistent patient outreach supported by patient communication apps, healthcare portal tools, active listening skills, effective communication frameworks, and empathy in healthcare administration. Better words often create faster payment.
EMR discipline matters just as much. If a patient gives new insurance over the phone and the update lives only in a message or loose note, the denial risk remains alive. If a referral arrives and gets scanned into the wrong document type, the office may technically have the proof but still lose time because nobody can find or trust it. If portal messages containing key coverage details never make it into the right workflow, the denial gets to repeat. That is why denial prevention depends on EMR integration tools, charting terminology, records release tools, healthcare CRM understanding, and medical office collaboration systems. The right fact in the wrong place still behaves like missing information.
There is also a patient-relations side to denial work that good offices take seriously. Patients already feel vulnerable when they need care. Adding a denial can make them feel blamed, trapped, or shut out. Strong medical admin assistants know how to explain payer-driven issues without sounding robotic, how to ask for missing documents without sounding accusatory, and how to keep the conversation moving when frustration rises. That is where de-escalation techniques, difficult conversation workflows, patient privacy communication guidance, front-desk process discipline, and scheduling conflict management become part of denial management too. Revenue recovery gets easier when patients cooperate instead of withdrawing.
5. How to Build a Denial-Resistant Office Process and Become More Valuable
The most valuable medical admin assistants do not just fix denials one by one. They look for patterns and redesign the workflow that keeps producing them. If the same payer denial appears every week, there is a process issue. If one clinic location keeps missing referrals, there is an ownership issue. If telehealth claims keep failing, the scheduling and eligibility logic need review. If patients keep arriving with outdated cards, reminder timing and message content need work. That kind of operational thinking aligns with medical administration technology reports, medical office automation trends, interactive healthcare administration reports, future-proof career planning, and top employer-desired CMAA skills. Pattern thinking is promotion-level thinking.
A denial-resistant office usually has a few shared traits. It verifies insurance close to the visit, uses clear referral and authorization trackers, confirms patient responsibility early, updates the EMR immediately when new information arrives, standardizes document labeling, monitors portal messages, and makes responsibility visible instead of assuming someone else will handle it. Those habits get stronger when teams compare their setup against secure scheduling platforms, EMR integration tools, patient communication directories, medical office staff scheduling tools, and medical admin workflow communities. Better systems produce better denials data because there are fewer mystery failures.
This is also career leverage. A medical admin assistant who can reduce denials, tighten intake quality, improve insurance capture, sharpen patient communication, and help teams act on recurring denial patterns becomes far more than a task performer. That person becomes somebody managers trust with access, workflow, and training responsibility. That path connects directly to CMAA certification value, career growth roadmaps, salary trend reporting, job market outlook, and healthcare efficiency research. Denial management is one of the clearest ways to prove you understand how the office really works.
6. FAQs About Denial Management for Medical Admin Assistants
-
A medical admin assistant can prevent many denials before they happen by strengthening patient intake, improving insurance verification, tightening appointment scheduling, updating the EMR accurately, and documenting clear next steps through front-desk workflows. Many denials begin in those exact areas.
-
Eligibility denials, demographic mismatches, referral problems, authorization gaps, wrong payer details, and communication-related delays are highly preventable when staff understand medical billing terms, insurance verification rules, healthcare portal workflows, patient communication tools, and front-desk process standards.
-
Start with clarity, not defensiveness. Explain what the payer issue is, what information is missing or conflicting, what you need from the patient, and what the next follow-up step will be. This works best when paired with active listening, de-escalation techniques, difficult conversation guidance, patient privacy communication, and effective patient communication terms.
-
Verify active insurance, payer order, subscriber details, referral status, authorization needs, guarantor accuracy, visit type, provider, and patient contact information. Those checks are strongest when supported by scheduling best practices, insurance verification workflows, secure scheduling tools, healthcare portal tools, and patient intake procedures.
-
A useful note states the denial issue, the source of the corrected information, the action taken, the proof attached, the date of follow-up, and the next owner. That approach becomes easier when staff understand EMR charting terms, healthcare CRM terminology, records release workflows, EMR integration tools, and privacy rules for patient communication.
-
Track repeats by payer, provider, location, service type, scheduler, and root cause. Then compare those patterns against intake quality, referral timing, auth workflows, document routing, and communication failures. That kind of review pairs well with medical office automation trends, medical administration technology reports, future-proof CMAA skill planning, medical office collaboration tools, and job-demand reports for medical admins.
-
Because knowledge without ownership still leaves gaps. Many offices know referrals matter, know eligibility matters, and know authorizations matter. The breakdown happens when nobody is assigned to trigger, track, verify, and close each step. Teams improve fastest when they combine front-desk workflows, staff scheduling systems, communication apps, healthcare CRM logic, and collaboration tools into one visible process.
-
Yes. Denial management proves that you understand revenue protection, patient communication, intake quality, documentation flow, and office process design. That combination supports advancement through CMAA certification value, career roadmap planning, salary trend reporting, job-market outlook, and healthcare efficiency research. It is one of the clearest ways to show operational maturity.