

Medical Scribe Certification FAQs: Your Complete Resource
Medical scribe certification gets confusing fast because candidates hear different advice from training programs, employers, hospitals, remote scribe companies, and pre-med peers. The real goal is simple: prove you can understand clinical language, follow provider reasoning, document encounters accurately, protect patient information, and work inside an EHR without becoming a liability. A strong study plan should connect medical terminology mastery, accurate clinical documentation, HIPAA compliance, and medical scribe career planning into one practical path.
1. What Medical Scribe Certification Actually Proves
A medical scribe certification is a job-readiness signal. It shows that you have studied the core language, documentation rules, workflow expectations, privacy responsibilities, and encounter structure that scribes use every shift. Employers still care about typing speed, professionalism, adaptability, and coachability, but certification gives your application a cleaner starting point when paired with medical scribe job interview preparation, medical terminology tutorials, EMR and charting terms, and documentation standards.
The strongest certification candidates understand what the exam is really testing. A scribe must listen for medically relevant facts, separate symptoms from diagnoses, document the provider’s assessment accurately, capture the plan without inventing clinical meaning, and leave a clean note that supports continuity of care. AAPC describes medical scribes as handling the documentation component so providers can focus on patient care, and its CPMS guidance emphasizes terminology, anatomy, medical record components, documentation requirements, HIPAA, billing practices, medico-legal risk, and E/M documentation knowledge. That connects directly to medical scribe impact on healthcare administration, medical scribe data accuracy, medical record compliance, and medical scribe efficiency tools.
The painful part is that many students study like they are memorizing a glossary. They can define “HPI,” “ROS,” “assessment,” and “plan,” then freeze when a provider speaks quickly, uses shorthand, jumps between complaints, or changes the diagnosis after reviewing labs. Certification prep should train judgment, not just recall. A candidate should know how to use top medical scribe documentation terms, must-know HIPAA terms, ICD-10 reference basics, CPT code awareness, and EHR platform familiarity under realistic pressure.
| # | Certification Question | Why It Matters | Best Next Step | ACMSO Resource |
|---|---|---|---|---|
| 1 | Start here Do I need certification? | Some employers train internally, while certification can help prove readiness before experience. | Compare job postings and identify repeated skill requirements. | Scribe careers with certification |
| 2 | Which exam should I choose? | Different credentials emphasize different experience levels, documentation depth, and eligibility rules. | Pick based on your background, target employer, and timeline. | Training courses and certifications |
| 3 | What does a scribe need to know? | Scribes must understand clinical flow, medical terminology, chart structure, privacy, and note accuracy. | Build a study plan around real encounter sections. | Documentation terms |
| 4 | How much terminology is enough? | Weak terminology slows you down and causes missed context during fast encounters. | Study prefixes, suffixes, body systems, abbreviations, and specialty terms. | Terminology mastery |
| 5 | Do I need anatomy? | Anatomy helps you follow complaints, exams, imaging, and provider reasoning. | Learn anatomy by complaint type rather than isolated diagrams only. | Memorize complex terms |
| 6 | Is HIPAA tested? | Privacy errors can damage patients, employers, and your credibility. | Study patient identifiers, minimum necessary use, access rules, and secure communication. | HIPAA compliance |
| 7 | What is the hardest exam skill? | Most candidates struggle with applying knowledge to messy clinical scenarios. | Practice notes from realistic encounter examples. | Realistic exam questions |
| 8 | How should I study EHR workflow? | Scribes work inside templates, sections, orders, messages, and provider preferences. | Learn common EHR sections and charting logic. | EMR and charting terms |
| 9 | Do scribes need coding knowledge? | Scribes usually do documentation support, but coding awareness helps avoid vague notes. | Learn the difference between documentation language and billing decisions. | CPT codes explained |
| 10 | Do I need ICD-10? | Diagnosis language appears constantly in assessment, history, and plans. | Learn how diagnosis terms appear in clinical documentation. | ICD-10 dictionary |
| 11 | How do I prepare for remote scribe jobs? | Remote roles require focus, clean written communication, and strong tech habits. | Practice asynchronous communication and digital workflow discipline. | Remote scribe market |
| 12 | Are emergency department scribes different? | ED scribes face speed, interruptions, acute complaints, and high documentation pressure. | Study chief complaints, time-sensitive plans, and concise note structure. | ED scribe roles |
| 13 | What if I want pediatrics? | Pediatric notes require guardian communication, age-specific history, vaccines, and development context. | Study pediatric workflows before applying to children’s clinics. | Pediatric scribe guide |
| 14 | Does telemedicine change documentation? | Virtual visits add consent, technology, location, and remote exam limitations. | Learn how telehealth changes note language and patient flow. | Scribes and telemedicine |
| 15 | How do I avoid over-documenting? | Too much irrelevant detail slows review and can blur clinical meaning. | Document what supports the visit, provider reasoning, and plan. | Documentation standards |
| 16 | How do I avoid under-documenting? | Thin notes can miss severity, duration, negatives, decision-making, and follow-up instructions. | Use a checklist for HPI, exam, assessment, and plan completeness. | Documentation compliance |
| 17 | Do I need typing speed? | Speed helps, but accuracy and clinical listening matter more under pressure. | Practice typing clinical phrases while preserving meaning. | Scribe efficiency techniques |
| 18 | How soon can I be job-ready? | Timeline depends on terminology base, documentation practice, and specialty exposure. | Use a structured study calendar instead of scattered review. | 30-day study schedule |
| 19 | How do I practice clinical scenarios? | Scenario practice builds judgment faster than passive reading. | Write sample notes from chief complaints and compare sections. | Interactive exam questions |
| 20 | Will certification help my resume? | Certification helps most when the resume proves workflow skills and documentation awareness. | Translate study topics into role-specific resume bullets. | Standout healthcare resume |
| 21 | How should I interview after certification? | Hiring managers want calm, specific answers about accuracy, feedback, and provider preferences. | Prepare stories about corrections, privacy, speed, and ambiguity. | Scribe interview prep |
| 22 | Can certification help pre-med students? | Scribing offers exposure to clinical reasoning, patient flow, and provider communication. | Choose roles that build learning without weakening documentation quality. | Scribe to physician journeys |
| 23 | What tools should I know? | Modern scribes may work with EHRs, dictation tools, AI tools, portals, and templates. | Learn tool categories and human verification responsibilities. | AI scribe tools |
| 24 | How do I handle provider preferences? | Providers differ in note style, phrasing, detail level, and workflow habits. | Ask clarifying questions, track preferences, and adapt without guessing. | Efficiency tools and techniques |
| 25 | What if I fail the first exam attempt? | A failed attempt usually means the study plan lacked scenario practice or weak-area review. | Audit missed domains, rebuild the schedule, and practice applied questions. | Pass certification first try |
| 26 | How do I choose employers after certification? | Different employers offer different pace, specialty exposure, training quality, and growth paths. | Target hospitals, urgent care, telehealth, specialty clinics, or pre-med pipelines intentionally. | Hospitals hiring scribes |
| 27 | Can scribes move into other roles? | Scribes can build toward clinical research, administration, coding awareness, or medical school pathways. | Track transferable skills from day one. | Scribe to CRC tracks |
| 28 | How do I keep skills sharp? | Documentation quality slips when scribes stop reviewing terms, standards, and feedback. | Create a weekly review cycle for terminology, note errors, and workflow lessons. | Certification FAQ resource |
2. Which Medical Scribe Certification Path Should You Choose?
Choose a certification path by matching three things: your current experience, your target role, and the type of documentation work you want to perform. A new candidate may need a beginner-friendly path that builds terminology, note structure, and HIPAA habits. An experienced scribe may need a more advanced credential that validates documentation depth, EHR fluency, and medico-legal awareness. That decision becomes easier when you compare medical scribe training courses, remote scribe opportunities, emergency department scribe roles, and medical scribe staffing agencies.
Two widely discussed credential paths are AAPC’s Certified Professional Medical Scribe and AHDPG’s Medical Scribe Certification Exam. AAPC’s help guidance states that CPMS applicants need two years of experience, which can combine medical and scribe experience, and that approved candidates take an online proctored exam. AHDPG states that its MSCE is a timed exam with 100 questions and 1 hour 15 minutes, with immediate pass/fail reporting and recertification by retaking the exam every two years. Candidates should always verify current rules directly with the credentialing body before paying, then align study with medical scribe exam questions, HIPAA for scribes, medical terminology mastery, and EHR charting terms.
The wrong path usually shows up as wasted time. A beginner buys an advanced exam before understanding encounter flow. An experienced candidate spends weeks reviewing definitions while ignoring applied documentation scenarios. A pre-med student picks the cheapest option without checking whether local hospitals value it. A remote-job applicant studies clinical vocabulary but ignores technology, privacy, and written communication. A smarter path starts with medical scribe career opportunities, top remote employers, telehealth scribe growth, and hospital hiring trends.
3. What You Need to Study Before the Exam
Start with the medical note. Every exam topic eventually points back to whether you can support a clear, accurate, provider-aligned chart. That means knowing the purpose of the chief complaint, HPI, ROS, past history, medications, allergies, physical exam, assessment, plan, discharge instructions, follow-up, and provider attestation. The candidate who understands structure can study faster because each term has a job. Build that foundation with documentation terms for scribes, medical documentation compliance, clinical documentation accuracy, and real-time documentation standards.
Next comes terminology. A scribe does not need to sound like a physician, but a scribe must recognize enough clinical language to avoid dangerous misunderstanding. “Denies chest pain,” “rule out pneumonia,” “history of uncontrolled diabetes,” “follow up if symptoms worsen,” and “provider discussed risks and benefits” all carry documentation weight. Study body systems, common abbreviations, diagnostic phrases, medication categories, procedure words, and specialty vocabulary through medical terminology tutorials, complex term memorization, ICD-10 terminology, CPT basics, and specialty documentation templates.
Then study privacy and workflow. A scribe sees sensitive information, hears sensitive conversations, and works near protected health information every shift. A weak candidate treats HIPAA as a test chapter. A strong candidate treats it as a daily behavior system: screen positioning, login discipline, patient identity, secure communication, minimum necessary access, and careful discussion of patient details. Use HIPAA compliance for medical scribes, must-know HIPAA terms, patient privacy communication, and legal responsibilities for healthcare admin roles.
4. How to Prepare for Medical Scribe Certification Without Wasting Weeks
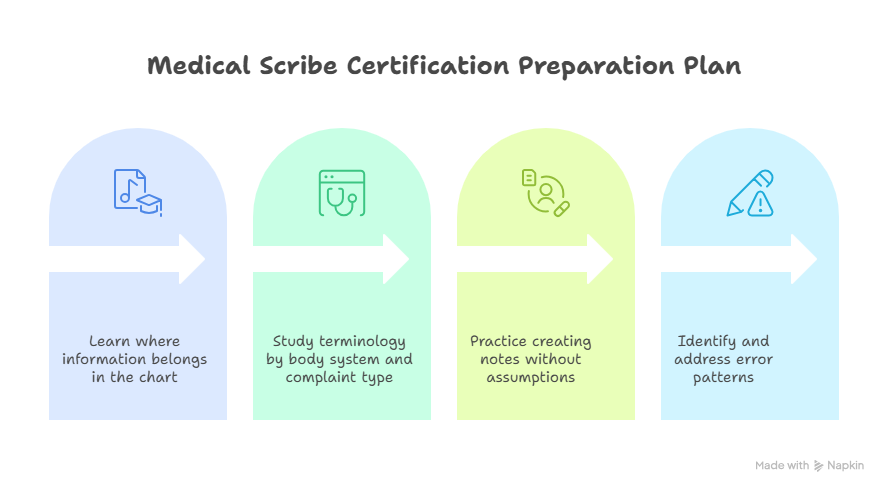
A strong prep plan uses blocks. Block one is note structure. Spend the first few days learning where information belongs in the chart. If you cannot place information correctly, more terminology will only create faster confusion. Practice by taking a sample complaint and sorting details into HPI, ROS, exam, assessment, and plan. This pairs well with realistic scribe exam questions, documentation terms, medical record accuracy, and clinical documentation compliance.
Block two is clinical language. Study terminology by body system and complaint type. For example, chest pain review should include cardiac, pulmonary, GI, anxiety, medication, family history, risk factors, red flags, and follow-up language. Abdominal pain review should include onset, location, radiation, nausea, vomiting, stool changes, urinary symptoms, pregnancy context where relevant, and surgical history. This method makes medical terminology mastery, ICD-10 code awareness, CPT code explanations, and specialty cheat sheets much easier to retain.
Block three is workflow simulation. Set a timer, read a short encounter, create a note outline, then check whether you captured the provider’s decision-making without adding unsupported claims. The most dangerous habit is filling gaps with assumptions. If the provider says “possible sinusitis,” the note should not transform it into a confirmed diagnosis. If the patient denies fever, that negative matters. If follow-up instructions are conditional, the condition must stay clear. Practice this with medical scribe efficiency techniques, medical scribes in emergency departments, telemedicine scribe workflows, and remote scribe market skills.
Block four is review. Many candidates review by rereading notes. Strong candidates review by finding error patterns: missed pertinent negatives, misplaced medications, weak assessment wording, incomplete follow-up, overlong HPI, vague plan language, and poor provider-preference adaptation. Create a mistake log and review it every two days. This is where 30-day certification study planning, first-try exam strategies, EMR charting terms, and HIPAA terms for scribes become daily tools.
5. How to Turn Certification Into Interviews, Better Notes, and Career Growth
Certification should change your resume language immediately. Replace vague claims like “good communication skills” with role-specific proof: documented patient encounters, understood medical terminology, maintained privacy standards, worked with EHR-style note structure, practiced HPI organization, and studied provider-facing documentation workflows. Hiring managers respond better when your resume reflects the actual job. Combine certification with medical scribe interview prep, medical scribe career pathways, top hospitals hiring scribes, and healthcare recruiters posting scribe roles.
In interviews, do not talk about certification like a badge you collected. Talk about what it trained you to notice. Explain how you separate patient-stated symptoms from provider assessment, how you handle uncertain terms, how you ask clarifying questions without interrupting care, how you protect patient information, and how you respond to feedback on note style. That kind of answer shows readiness for provider documentation support, documentation compliance standards, EHR platform workflows, and clinical documentation accuracy.
The broader career outlook favors people who can adapt as healthcare documentation changes. BLS projects medical assistant employment to grow 12% from 2024 to 2034, with about 112,300 openings per year, and notes that medical assistants perform administrative and clinical tasks such as scheduling appointments, entering patient information into medical records, coding information, and contacting insurance companies about billing. While medical scribes have their own role identity, these surrounding healthcare support trends matter because documentation, EHRs, patient flow, billing awareness, and compliance keep moving closer together. That makes medical scribe job growth reports, medical scribe employment trends, salary analysis for certified scribes, and medical scribe impact on hospital revenue useful beyond exam prep.
Certification can also support long-term movement. Some scribes use the role as pre-med exposure. Some move toward clinical research, medical administration, coding, care coordination, telehealth operations, or EHR optimization. The key is to track the skills you build: accuracy under pressure, clinical listening, provider communication, privacy discipline, and workflow improvement. Those skills connect naturally to scribe-to-physician journeys, clinical research sites hiring scribes, medical admin technology trends, and AI medical scribe tools.
6. FAQs: Medical Scribe Certification
-
Many employers hire and train new scribes internally, but certification can strengthen your application when you lack experience, want remote work, or need proof that you understand documentation basics. The best approach is to study target job postings, then match your preparation to the skills employers keep repeating. Start with medical scribe careers with certification, top medical scribe training courses, medical scribe job interview prep, and realistic scribe exam questions.
-
The best certification depends on your experience level, target employer, budget, study timeline, and whether you want entry-level proof or advanced documentation validation. Experienced candidates may explore credentials with stricter eligibility, while beginners may need structured training first. Compare current requirements directly through credentialing bodies, then study with documentation terms for scribes, medical terminology tutorials, HIPAA compliance guidance, and EMR charting terms.
-
High-value study areas include medical terminology, anatomy basics, chart structure, HPI organization, ROS language, physical exam documentation, assessment and plan flow, HIPAA, EHR navigation, provider communication, and medico-legal awareness. The practical goal is to document what happened accurately, clearly, and within your role. Strengthen your foundation with medical documentation compliance, clinical documentation accuracy, medical terminology mastery, and HIPAA terms for scribes.
-
A candidate with healthcare experience may need a shorter review period, while a beginner often needs several weeks of structured terminology, charting, and scenario practice. The most efficient plan uses daily note-structure drills, body-system vocabulary, HIPAA review, and timed clinical scenarios. Use 30-day certification study planning, first-try certification strategies, complex medical term memorization, and realistic exam questions.
-
Medical scribe certification can help pre-med students enter clinical environments with stronger documentation awareness and better vocabulary. The bigger value comes from doing the role responsibly: listening carefully, respecting patient privacy, learning provider reasoning, and understanding how care decisions appear in records. Explore scribe-to-physician journeys, hospitals hiring scribes, pre-med gap-year programs, and academic medical centers using scribes.
-
Common mistakes include memorizing terms without practicing note placement, ignoring HIPAA until the end, studying coding too deeply while neglecting clinical documentation, skipping timed practice, and assuming every provider phrase belongs in the note exactly as heard. Build a cleaner plan through medical scribe exam questions, documentation standards, EMR charting terms, and medical terminology mastery.