

What Scribes Do: Their Roles And Impact On Healthcare In 2025

A medical scribe, also known as a medical transcriptionist, is a healthcare professional who assists physicians in managing electronic health records (EHR) and handling clerical documentation. Their role includes recording patient visit details, organizing medical data, and working closely with physicians to ensure efficient and accurate healthcare delivery. Medical scribes gather billing data, process insurance information, and record patient interactions. Their specific responsibilities may vary depending on the physician and medical facility, with some focusing primarily on data entry and record-keeping, while others work more directly with physicians during patient consultations. This role is an excellent way for aspiring medical professionals to gain hands-on experience in the healthcare industry, offering direct exposure to the daily duties of doctors, patient care, and medical terminology.
Why Healthcare Needs Scribes Now More Than Ever
The healthcare industry’s growing dependence on technology has drastically changed the way healthcare services are delivered. The introduction of electronic medical records (EMR or EHR) has improved cost, access to information, and patient care. However, the switch from paper charts to digital records, mandated by recent regulations, has reduced the need for traditional transcriptionists, who once converted paper charts into digital form. Physicians must now report quality codes for most patients to track their conditions and treatments, which adds to their administrative workload. Scribes play an essential role in easing this burden, helping healthcare professionals maintain accurate, up-to-date patient records and comply with these new requirements.
Medical Scribes in Clinics
In clinic settings, medical scribes perform a broad range of tasks compared to their counterparts in hospitals. With a slower pace and more stable patients, scribes in clinics handle various documentation duties such as entering quality codes, inputting orders, and recording charges, all under close physician supervision. This setting offers valuable exposure to medical decision-making, especially for those aspiring to pursue advanced healthcare careers. Scribes in primary care, such as family medicine and internal medicine, also ensure preventive tests, such as colonoscopies and mammograms, are up-to-date. Depending on the specialty, documentation requirements can vary, making the role highly versatile across different medical fields.
Medical Scribes in Hospitals
In hospitals, scribes are predominantly found in emergency rooms (ERs), although they can also work in other areas. The work pace in the ER is much faster and more intense than in a clinic. Scribes in the ER focus primarily on recording patient information under pressure, ensuring that the doctor can focus on the patient rather than administrative tasks. They also assist by tracking test results and informing the physician when results come in, which helps in decision-making during critical situations.

Responsibilities of a Medical Scribe
Medical scribes play an essential role in healthcare, managing EHR systems and assisting with various administrative tasks. Some of their main responsibilities include:
Managing EHR: Scribes ensure that medical histories, test results, and treatment plans are accurately entered into the EHR system, providing physicians with quick access to patient information for decision-making.
Documenting History of Present Illness (HPI): They record detailed information about the patient's symptoms, the illness's duration, and other relevant details to aid in diagnosis and treatment.
Transcribing Physician’s Dictation: Scribes transcribe dictations made by physicians, ensuring that medical records are clear, accurate, and complete.
Drafting Medical Correspondence: They also prepare referral letters, consultation requests, and other forms of communication to coordinate care with specialists and other providers.
Assisting in the ER: In emergency settings, scribes are vital in documenting discharge details, writing prescriptions, and tracking consultant call-backs, helping physicians handle a high volume of patients efficiently.

The Growing Role of Digital Scribes
With the advent of AI-powered systems, digital scribes are becoming increasingly common. These systems automatically convert spoken words into structured medical notes, reducing the reliance on human scribes. This transition has led to improved accuracy in medical documentation and greater efficiency in updating patient records. Digital scribes also improve physician-patient interaction by reducing the time spent on documentation, allowing healthcare providers to focus more on patient care. PubMed.
Challenges and Solutions with Digital Scribing in 2025
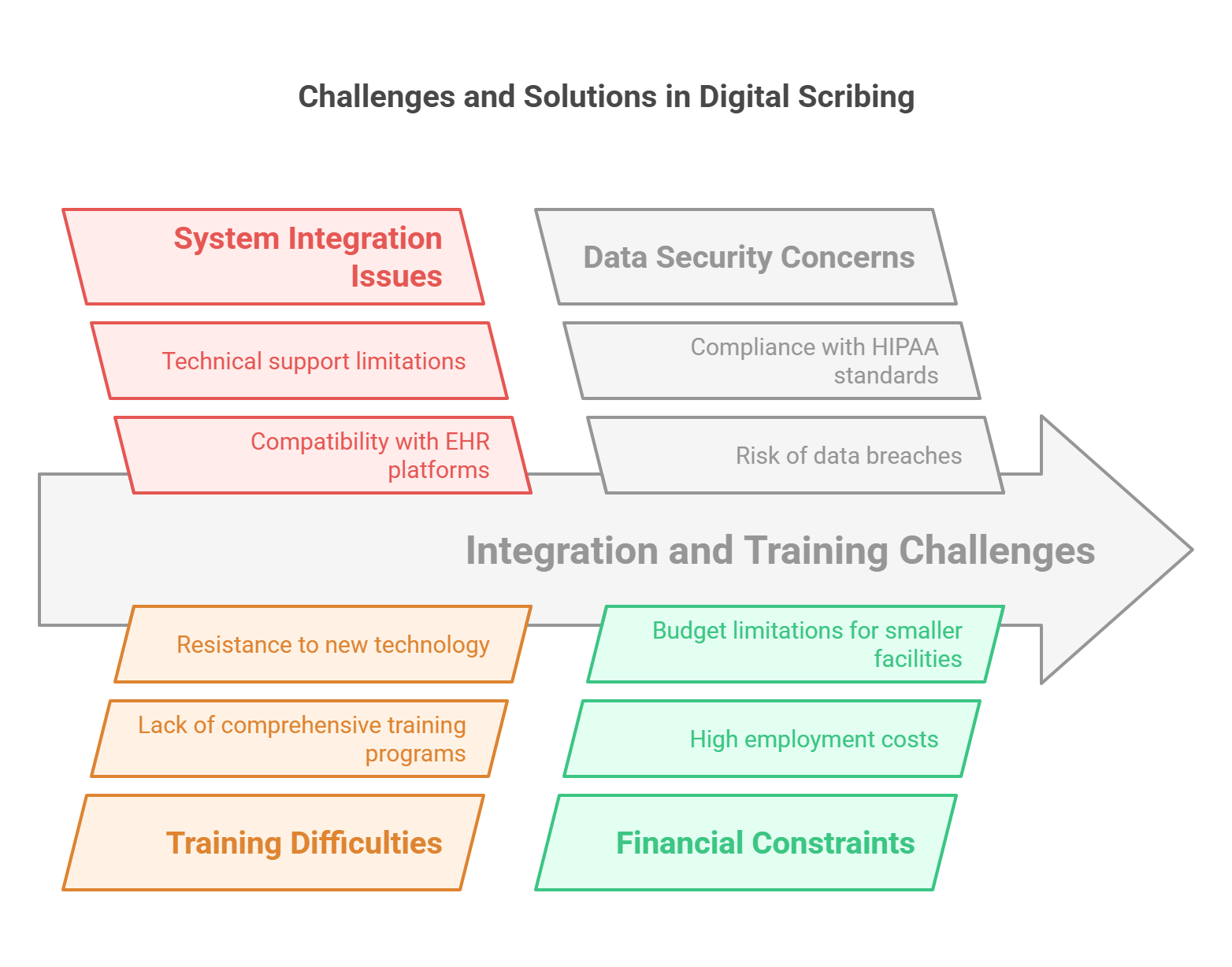
While digital scribing brings many advantages, it also presents challenges. Some limitations include issues with integrating digital systems with other EHR platforms, difficulties in training clinicians to use these systems, and concerns about data security. Healthcare facilities are addressing these challenges by offering better training programs, improving system compatibility, and ensuring that digital scribing technologies comply with HIPAA standards.
Importance and Limitations of Medical Scribes
Medical scribes help reduce physicians' administrative workload, enhancing overall healthcare efficiency and patient care. They are invaluable in helping doctors focus on diagnosis and treatment rather than documentation. However, the role comes with limitations, such as the time-consuming nature of training and the potential for high turnover, as many scribes use the position as a stepping stone to medical school or other healthcare careers. Furthermore, the financial costs of employing scribes can be significant, particularly for smaller healthcare facilities. American Medical Association.
Less Known Facts About Medical Scribes (2025)
The rise of digital scribes has significantly reduced human error in medical documentation, improving the accuracy of patient records.
Many medical scribes transition into healthcare roles such as medical assistants, nurse practitioners, and even physicians, with the experience providing valuable insights into clinical workflows.
Research shows that physicians who use scribes report lower levels of burnout due to reduced documentation workload, leading to better job satisfaction.
Scribes working in academic settings, such as teaching hospitals, also assist medical students and residents by ensuring smooth documentation during clinical training.
Digital scribes are expected to become even more prevalent in the coming years, especially with advancements in AI that allow for real-time documentation and decision support.
Scribes can also play a crucial role in telemedicine, helping physicians document virtual patient visits and improve the quality of care remotely.
conclusion
Medical scribing is a vital role in modern healthcare, bridging the gap between physicians and administrative tasks. By accurately documenting patient interactions, scribes enhance efficiency, improve doctor-patient relationships, and reduce medical errors. ASMSO plays a crucial role in shaping the standards and training for medical scribes, ensuring high-quality documentation and support in clinical settings. This career path offers invaluable hands-on experience for those aspiring to enter the medical field, providing a strong foundation in clinical operations and medical terminology. With growing demand, evolving technology, and opportunities for career advancement, medical scribing remains an excellent stepping stone into the healthcare industry. Whether as a long-term profession or a gateway to further medical education, becoming a medical scribe is a rewarding and impactful choice.
FAQs about Medical Scribes (2025)
-
A medical scribe works alongside physicians, directly documenting patient visits and managing EHRs, while a medical transcriptionist primarily focuses on transcribing dictated medical reports into written form.
-
While certification is not mandatory, many scribes choose to pursue certification to enhance their qualifications and career prospects. One popular option is the Certified Medical Scribe Specialist (CMSS) certification.
-
Digital scribes use AI-powered systems to automatically convert spoken words into structured medical notes, reducing errors, improving efficiency, and allowing physicians to spend more time with patients.
-
Yes, medical scribes must have a solid understanding of medical terminology, procedures, and documentation protocols to accurately record patient information.
-
Some challenges include integration with existing EHR systems, the need for clinician training, and data security concerns. However, these challenges are being addressed with better technology and training programs.